Factors affecting Carpal Tunnel Syndrome in End Stage Renal Disease with maintenance Hemodialysis: A systematic review
Abstract
Introduction: The number of patients with End Stage Renal Disease (ESRD) is increasing every year, as well as those who have to undergo hemodialysis. Most hemodialysis must be undertaken in a long time. Long term hemodialysis is known to be associated with the incidence of Carpal Tunnel Syndrome (CTS). Method: This study aimed to systematically review factors contributing in the mentioned problem. Literature research was done using three search engines, consist of Google Scholar, Pubmed and ProQuest. Journals used are limited to the last 5 years or those deemed to be relevant. The studies obtained were further read and appraised critically. Result and Discussion: From a total of 423 journals, 4 articles were selected based on inclusion and exclusion criteria. The prevalence of CTS was found to be higher in ESRD patients undergoing maintenance hemodialysis (MHD). Age, Gender, MHD Duration, β2-Microglobulin are factors that have long been known to play a role. Several other factors such as serum prealbumin, serum albumin, Blood Lead Levels, hepatitis infection, wrist injury, predialytic urea serum and BMI have been implicated in the incidence of CTS in ESRD patients undergoing MHD in some literatures. Conclusion: The factors mentioned earlier were found to have different roles and it is interesting for further reviewed. However, unfortunately there is still very little research that discuss these matters and more research needs to be done related to the factors above.
Keywords
Chronic Kidney Disease, Hemodialysis, Carpal Tunnel Syndrome, Dialysis Related Amyloidosis
INTRODUCTION
Carpal Tunnel Syndrome (CTS) is a common peripheral neuropathy with a variety of risk factors 1, 2. Some studies mentioned the prevalence of CTS in Europe is between 1% and 7% 3, 4, 5, 6. On the other side, the study by Atroshi et al which compared CTS in the general population in Sweden and in the US had results of 324 cases per 100,000 people vs 542 cases per 100,000 people in the female population and 125 cases per 100,000 people vs 303 cases per 100,000 people in the male population 2, 6. Cohort retrospective study in Taiwan calculated the incidence and risk of CTS in End Stage Renal Disease (ESRD) patients undergoing Maintenance Hemodialysis (MHD) found that the results in the control group were CTS patients without ESRD with 540 cases per 100,000 patients per year 7. Symptoms of CTS are tingling, pain in the wrist, hypesthesia at the distal end of the sensory innervation of the median nerve, and decreased grip strength. Abnormalities such as hypotrophy or even atrophy of the thenar muscles can be found in severe cases 8.
Patients with ESRD who underwent MHD were said to be predisposed to develope CTS and were first reported in a case report by Jain et al 9. CTS is said to occur in about 30-50% of ESRD patients who have had MHD for more than 10 years and more than 80% in patients who have had MHD for more than 30 years. There are specific factors contributing to the development of carpal tunnel syndrome in ESRD patients undergoing MHD, one of them is β2-microglobulin (β2-M) fiber deposits which associated with inflammation and oxidative stress 10, 11, 12, 13. Deposition of β2-M will induce the activation of proinflammatory factors such as interleukin-1 (IL-1), tumor necrosis factor-a (TNF-a) and transforming growth factor b (TGFβ). (14)Another factor that is said to be influential is arteriovenous fistula (AV) 11, 12, 14.
Treatment of CTS can be either conservative or surgical depending on the severity of the disease, the patient's preferences and the surgeon's abilities 15. With some of the considerations above, carpal tunnel decompression is the most commonly performed surgical procedure with patient satisfaction rates of up to 90% 16, 17. Research by Tsai et al also showed that CTS patients in ESRD who underwent MHD were more likely to undergo surgery than the control group (62.4% vs 12.9%). This is because patients with ESRD who undergo MHD generally experience decreased motor and sensory abilities or electrophysiological abnormalities that do not improve with conservative treatment 15.
CTS condition can cause a decrease in the ability of ESRD patients to carry out daily life activities 18. Therefore, an early detection of the incidence of CTS in ESRD patients who routinely undergo MHD can help determine the severity and prevent permanent median nerve damage and improve the patient's quality of life 15. Hence, it is necessary for the physicians and researchers to investigate the risk factors associated with CTS in patients with ESRD undergoing MHD.
METHOD
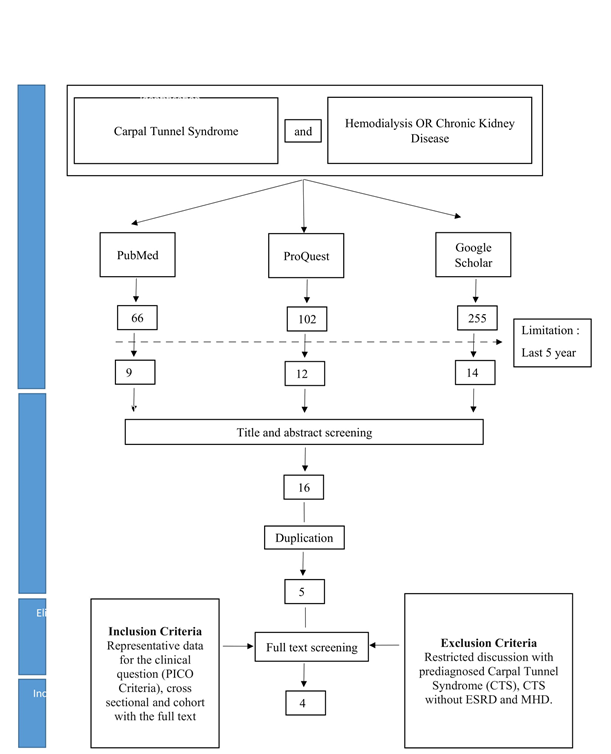
The literatures search study were conducted using three electronic databases, namely PubMed, ProQuest and Google Scholar. Literatures search are limited to journals that can be accessed in the last 5 years or> 5 years considered relevant. The studies are searched by using the Boolean system which can be seen in Table 1 .
|
Database |
Keywords |
Result |
|
PubMed |
((Carpal Tunnel Syndrome) OR (CTS) AND ((Hemodialysis) OR (Chronic Kidney Disease)) |
66 |
|
ProQuest |
((Carpal Tunnel Syndrome) OR (CTS) AND ((Hemodialysis) OR (Chronic Kidney Disease)) |
102 |
|
Google Scholar |
((Carpal Tunnel Syndrome) OR (CTS) AND ((Hemodialysis) OR (Chronic Kidney Disease)) |
255 |
Literature search study on each database was used to search for related journals that describe the incidence of Carpal Tunnel Syndrome (CTS) in End Stage Renal Disease (ESRD) patients undergoing Maintenance Hemodialysis (MHD). Associated studies include studies that describe clinical questions with full-text articles available with cross-sectional and cohort study types. Abstract and title screening were performed using inclusion criteria with PICO criteria according to the following details (P: Patients with End Stage Renal Disease, I: Maintenance Hemodialysis, C: none, O: Carpal Tunnel Syndrome). Existing exclusion criteria were case discussion limited to prediagnosed CTS, CTS without ESRD and MHD. The studies that have been obtained are read further and appraised critically. The critical appraisal was conducted based on the Oxford's Center for Evidence-Based Medicine. 19
RESULTS
The results obtained from three database searches showed that there were 423 related journals explain the factors that play a role in the incidence of CTS in ESRD patients undergoing MHD. Each journal is described and divided into several groups, one of which is dividing the two groups with the details of the ESRD patient group who underwent MHD and the group without a diagnosis of kidney disease. A total of 4 selected articles were analyzed and further discussed to answer the clinical questions made, and then a critical appraisal was conducted. PRISMA flowchart and critical analysis can be seen in Figure 1 and Table 2.
A retrospective cohort study by Tsai et al in Taiwan on 17,692 ESRD patients undergoing MHD showed that CTS occurred in 1,095 patients (6.19%). The incidence of CTS in ESRD patients undergoing MHD was 975 cases per 100,000 patients per year, higher than the control group at 540 cases per 100,000 patients per year. Male patients over 50 years of age had a greater 10 year cumulative incidence, which are 5.13% vs 3.30%. In female patients over 50 years of age there were also a higher cumulative incidence of 8.62% vs 7.85% 15. Study from Kuharic et al in Croatia on 78 MHD patients showed that the risk of CTS which was screened using Levine questionnaire to detect how high the risk of CTS based on the symptoms experienced by patients including pain, paraesthesia, loss of sensation, weakness, nocturnal symptoms and functional status found in 30 patients (38.5%) 20, 21. A study by Dung et al in Vietnam on 373 ESRD patients undergoing MHD showed that CTS occurred in 44 patients (11.8%). The mean age of the patients was 45.6 years with a range of age 40.1-64.22 years with 57.4% male 22. Research by Huang et al on 866 MHD patients showed that the results of CTS occurred in 76 patients (8.8%) with a mean patient age of 56 years and more men, namely 50.8% 23.
Furthermore, study by Nishi S et al diagnosed CTS based on clinical assessment by physicians which is similar to that of Kuharic et al in their study that detected the risk of CTS based on a questionnaire 20, 24. Moreover, in the study of Tsai et al, CTS was diagnosed based on signs and symptoms either supported by an electrophysiological test or not 7. These factors allow for bias in the studies. In contrast to that, research by Dung et al diagnosed CTS according to the American Academy of Orthopedic Surgeons, where in addition to signs and symptoms, nerve conduction examinations were also carried out 22, 25 It was likewise with the study by Huang et al that diagnosed CTS based on clinical and electrophysiological examination 23.
Electrophysiological examination was able to exclude the possibility of bias, for instance, it was showed in the study of Huang et al from total of 234 (27.6%) patients with clinical CTS, after electrophysiological examination there were reduced to 76 (8.8%) patients 23. Besides, research by Kuharic et al showed that there was no statistically significant relationship between the hand with CTS symptoms and the hand with vascular access for hemodialysis. This helps rule out the possibility that the cause of the patient's symptoms is CTS, not complications from vascular access such as catheter arteriovenous fistulas, arterial steal syndrome or venous hypertension 11, 21.
The number of comorbidities found in study by Tsai et al were hypertension, diabetes mellitus, COPD, stroke, peripheral vascular disease, rheumatoid arthritis, myocardial infarction, and wrist injuries. However, the study did not explain what are the main causes of patients experiencing ESRD to undergo MHD 7. In contrast to that, a study by Kuharic et al states that sequentially patients who have symptoms lead to CTS with MHD starting with the most ESRD caused by diabetic nephropathy 10 (33.3%), interstitial nephritis 8 ( 26.7%), glomeluronephritis 5 (16.7%), hypertension 5 (16.7%), and others as much as 2 (6.7%). (21). Next is the study by Kopec et al that found that most ESRD patients who underwent MHD were sequentially due to glomerulonephritis (45%), renal chirrhosis of uknown origin (20%), degeneration polycystic kidney disease (12.5%), chronic pyelonephrisits (10%), and diabetic nephropathy (5%), amyloidosis nephropathy (2.5%), and hypertensive nephropathy (2.5%) 26.
DISCUSSION
Along with the increasing prevalence of patients with ESRD, the need for dialysis is as well increasing every year, including from a financial perspective. Data from the United States Renal Data System in 2018 shows that the incidence of ESRD in 2018 was 131,636 per one million population, an increase of 2.3% since 2017. The number of patients undergoing hemodialysis ranged from 111,000 to 113,000 for four consecutive years until 2018 27. One of the diseases that arise as a result of undergoing hemodialysis is CTS 9. CTS will be more run the risk in ESRD patients undergoing MHD, this is attested by the following study, one of which is the retrospective cohort Tsai et al in Taiwan in 17,692 patients showing that ESRD patients with MHD have 14 times the risk of developing CTS compared with control patients, namely patients without ESRD and MHD. (7)Gender
Gender is one of the factors that increase the risk of developing CTS in ESRD patients undergoing MHD. Gender found to play a role is in women, which is reported by research by Tsai et al and Dung et al. (7,23)The mechanism that causes women to be a factor is substantiated by the study of Mitake et al, which explains menopause and hormone factors as the cause 28.
Age
Another factor that is said to play a role is age. Several studies suggest that age> 50 years increasing the risk of developing CTS as described in the study of Tsai et al (aged 50-59 years), Kuharic et al and Dung et al (> 50 years) 7, 20, 22. In this case, age can be influenced by the time patient start hemodialysis or by the long duration of hemodialysis which will be described next.
Duration of MHD
Apart from gender and age, the duration for which patients undergo MHD also plays an important role in the development of CTS. The duration plays a role due to the β2-M deposition factor, where the longer a person has to undergo MHD, the higher the likelihood of developing CTS due to the accumulation of β2-M 10, 11, 12, 13, 14. The study conducted by Tsai et al was not explaining in detail about the cause or use of the MHD device used by each patient, however, the duration of patients undergoing MHD with the cumulative incidence of CTS was found increase sequentially every 2 years, from 2 years to 10 years, namely 1.4%, 2.7%, 3.9%, 5.7% and 8.0% with p values = <0.0001 7.
This is espoused with the study by Kuharic et al that showed the risk of developing CTS was more frequent in patients with longer MHD and not influenced by the cause of ESRD 20 Study by Dung et al also showed that ESRD patients who underwent MHD with CTS versus without CTS had 9.5 years of MHD duration versus 3.3 years of MHD duration. (Nguyen et al, 2020) This is similar to the study by Huang et al (12.3 years vs 6.4 years) 29.
β2-Microglobulin
The next factor said to play a role in causing CTS in ESRD patients undergoing MHD is β2-M. Research by Dung et al showed that β2-M concentrations were higher in patients with CTS than in the control group (82.45 mg / L vs 64.1 mg / L) 22. Research by Nishi et al showed that the use of β2-M adsorption columns can control joint pain with good efficacy. 24. Although the pathophysiology is still unclear, the β2-M adsorption column is thought to play a role in reducing cytokine levels 30, 31. It is well known that β2-M plays a role in the activation of pre-inflammatory factors and oxidative stress 10, 11, 12, 13, 14.
This can be explained that most of β2-M is usually excreted via the kidneys. Yamamoto, 2011 Unfortunately, there will be impaired filtration and insufficient catabolism in patients with ESRD, resulting in continuous production and intradialytic production due to membrane incompatibility, all of which can lead to an increase in serum β2-M concentration 20. Normal values of serum β2-M is ranged between 1 and 3 mg / L, whereas these values can exceed 100 mg / L in patients with ESRD and in patients with chronic hemodialysis 32.
Others
It is interesting that in each study other factors were found to be influential apart from those mentioned above. As in Dung et al study, which showed that prealbumin serum was better than serum albumin to predict the incidence of CTS in MHD patients. With the results of the prealbumin value <30 mg / dL has a sensitivity and specificity of above 70% 22. Slightly explained, prealbumin is a liver secretory protein used to assess malnutrition in patients with chronic disease, including patients with MHD 33. Prealbumin assessment may also indicate a systemic inflammatory process in dialysis patients. The liver increases prealbumin synthesis when the body experiences inflammation to boost the immune system to protect the body from inflammatory stimuli, especially in patients with acute inflammation 22.
Meanwhile, a study by Huang et al found that serum albumin <4 g / dL was a significant factor in the incidence of CTS in MHD patients 23. A similar thing was also reported by Lukowsky et al, which showed that serum albumin was a predictor of CTS in ESRD patients undergoing MHD, where it is indicating malnutrition and an increase risk of inflammation 34.
In addition to the two factors above, the value of Blood Lead Levels (BLL)> 12.3 microg/ dL according to Wen Hun et al is said to be able to predict the incidence of CTS in MHD patients 23. The increase in lead due to environmental exposure directly has a calcifying effect in connective tissue 10. This allows calcification in the carpal tunnel leading to CTS 23. Indirectly, lead will cause liver damage through TNF-a and oxidative stress. (36)Lead damages cells through the increase of oxidative stress and -OH free radicals through the Fenton reaction 35. Lead can also cause β2-M deposition in the carpal tunnel indirectly via TNF-a 23.
Other factors that influence the incidence of CTS in ESRD patients undergoing MHD are hepatitis infection, wrist injury and BMI. Hepatitis virus infection is said to have a statistical effect according to the research of Dung et al and Huang et al. Where in Dung et al's study showed that the prevalence of hepatitis was higher in CTS patients with ESRD than in the control group (68.4% vs 24.3%) 22. The univariate logistic regression analysis in Huang et al's study showed that patients with positive HCV were 2 times more likely to develop CTS with p = 0.006 23. History of wrist injury is a factor that is said to be significant according to the research by Tsai et al. However, this study does not mention what type of wrist injury was experienced by the patients 7. Research by Kuhari et al shows that the influencing factors are predialytic urea serum and BMI, in which the study said that every 1 mmol / L increase increases the risk of CTS by 10.8%. The mean BMI of CTS patients with ESRD who underwent MHD was 27.6 kg / m2 versus 25.1 kg / m2 in the control group. However, in this study, the average BMI of all patients was already high, which was 26.1 kg / m2 20. There are no studies yet that explain the mechanism by which CTS occurs in ESRD patients undergoing MHD related to the other factors above.
CONCLUSION
Knowing the risk of CTS in ESRD patients undergoing MHD, early clinical examination and electrophysiological testing are necessary. This is useful for determining early treatment and preventing permanent damage to nerves. This study summarizes and systematically discusses the factors that influence the incident in selected journals for the benefit of further research and clinical decisions. The factors that influence and are discussed in almost all of these journals are gender, age, duration of MHD and β2-M, therefore we think this does not need to be discussed in subsequent studies. Factors that we think need further research are serum prealbumin, serum albumin, BLL, hepatitis infection, history of wrist injury, predialytic urea serum and BMI to determine whether the above factors have an important role in the development of CTS in ESRD patients undergoing MHD.
DISCLOSURES
Conflict of Interest
The author reports no conflicts of intereset in thist work.
Funding Source
None
Author Contribution
All authors contribute in concepting, designing, conduct the study, prepare the manuscript and agree for this final version of manuscript to be submitted to this journal.
Acknowledgments
The Authors are responsible for this study and also reports there is no conflicts of interest in this work.
|
First author and year |
Study size and settings |
Study design |
Study period |
Population |
Outcomes |
Factors Affecting CTS in ESRD with MHD |
|
Tsai, 2020(7) |
17,692 patients with ESRD on dialysis 176,920 patients without diagnosis of kidney disease, Taiwan, National Health Insurance Research Database (NHIRD) |
Retrospective Cohort study |
January 2003 to December 2012 |
ESRD on dialysis and patients without diagnosis of kidney disease |
Cohort With CTS= 1095 (6.19%) Without CTS= 16,597 (93.81%) Control With CTS= 9040 (5.11%) Without CTS= 167,880 (94.89%) CTS Incidence Rate 975.84/100.000 Incidence Rate Ratio 1.79 95% CI 1.68-1.91 Risk of CTS HR 13.95 95% CI 10.95-17.76, P< 0.0001 |
Age HR 1.02 95% CI 1.02-1.02 p< 0.0001 Gender Female/male HR 2.56 95% CI 2.45-2.68 p< 0.0001 Duration of MHD Every 2 years from years 2-10 cumulative incidences of CTS in the ESRD on dialysis cohort vs control 1.4% vs 0.8%, 2.7% vs 1.8%, 3.9% vs 2.9%, 5.7% vs 4.4%, and 8.0% vs 5.1%, all p<0.0001 Wrist Injury Cohort= 555 (3.13%) Control= 8548 (4.83%) HR 1.23 95%CI 1.13–1.34 p< 0.0001 |
|
Kuharic, 2019(21) |
78 patients at Department for Nephrology in University Hospital Osijek |
Cross-Sectional Study |
2018 |
Patients with ESRD on chronic Hemodialysis |
Patients ESRD on MHD at risk of CTS = 30 (38.5%) Age Risk of CTS= 70 (62-81) years Without risk= 65 (55-73) years Gender Risk of CTS Male= 18 (60%) Female= 12(40%) Without risk Male= 32 (66.7%) Female=16 (33.3%) |
Age each year of age increasing risk of CTS by 6.9% OR 1.069 95%CI 1.017-1.123 p= 0.008 Duration of MHD (years) Risk of CTS= 4 (2-7) Without Risk = 3 (1-5) Predialytic Urea Serum each mmol/L increasing risk of CTS by 10.8% OR 1.108 95%CI 1.007- 1.219 p= 0.035 BMI each kg of body mass increasing risk of CTS by 15.7% OR .157 95%CI 1.031- 1.3 p= 0.013 |
|
Dung, 2020(23) |
373 patients at Hemodialysis Center, Bach Mai Hospital, Ha Noi, Vietnam |
Cross-Sectional Study |
March 2016 |
End Stage Renal Disease (ESRD) patients with Maintenance Hemodialysis (MHD) using low flux dializer |
CTS= 44 (11.8%) Age (Mean ± SD) years CTS= 52.16 ± 12.6 Without CTS= 44.74 ± 14.44 p< 0.001 |
Gender (Female) HR 5.918 95% CI 1.844-18.989 p= 0.003 Duration of MHD HR 1.04 95% CI 1.023-1.058 p<0.001 Prealbumin cutoff value 26.5 mg/dL Sensitivity= 72.7% Specificity= 79.9% β2-M cutoff value 78.85 mg/L Sensitivity= 65.9% Specificity= 78.7% Hepatitis Infection CTS= 36 (81.8%) Without CTS=119 (36.17%) |
|
Huang, 2019(24) |
866 patients from 3 HD centers of Linkou, Taipei, and Taoyuan Chang Gung Memorial Hospitals |
Multicenter Cross-Sectional Study |
2016 |
Patients >18 year old who had received HD > 6 months |
Clinical CTS = 234 (27.02%) Confirmed CTS = 76 (8.8%) Age (Mean± SD) 56.18 ± 13.59 With CTS 57.36 ± 12.46 Without CTS 56.07 ± 13.69 Gender Male= 440 (50.8%) Female= 426 (41.9%) With CTS Male= 35 (46.1%) Female=41 (53.9%) Without CTS Male= 405 (51.3%) Female=385 (48.7%) |
MHD Duration OR 1.203 95% CI 1.138-1.273 p< 0.001 Albumin < 4g/dL OR 2.221 95C% CI 1.284-3.842 p= 0.004 BLL > 12.3 microg/dL OR 6.287 95% CI 3.737-12.472 p< 0.001 Sensitivity= 79% Specificity= 69% HCV Infection OR 2.07 95% CI 1.23- 3.47 p= 0.006 |